How to Handle RPM Data Volume at Enterprise Scale
How to handle RPM data volume at enterprise scale, from alert design and FHIR ingestion to data quality controls for health IT and telehealth operations teams.
How to Handle RPM Data Volume at Enterprise Scale
Handling RPM data volume at enterprise scale stops being a device problem pretty quickly. It becomes an operations problem, an integration problem, and, if the program grows fast enough, a trust problem. Health systems can launch remote patient monitoring with a few hundred patients using manual review and lightweight alerting. That same model starts to break when thousands of patients are transmitting readings into EHR-connected workflows every day. The bottleneck is rarely raw storage. It is deciding what deserves clinical attention, what should be summarized, and what has to move into the record in a standardized way.
"The remote monitoring programs in the study did not follow clear PGHD management or quality assurance approach." That was the conclusion reached by Robab Abdolkhani, Kathleen Gray, Ann Borda, and Ruth DeSouza in JAMIA Open (2019) after interviewing 20 experts involved in remote monitoring programs.
Enterprise RPM data volume is mostly a workflow problem
At small scale, RPM teams can tolerate inconsistency. At enterprise scale, inconsistency compounds. One device vendor sends hourly readings, another sends event-driven transmissions, and a third batches overnight. One service line wants every value in the chart. Another only wants exception-based documentation. Meanwhile the telehealth team is trying to preserve response times without turning nurses into inbox managers.
Three pressure points usually show up first:
- Too many transmissions reaching clinical staff without triage
- Too much variation in data quality across devices, patient behavior, and vendor feeds
- Too many integration pathways between device platforms, middleware, and EHR workflows
A 2025 framework study in JMIR Medical Informatics by Job van Steenkiste and colleagues examined one year of hypertension telemonitoring data at Maasstad Hospital specifically to analyze alert burden and processing load. Their premise was blunt: telemonitoring can improve efficiency, but alert handling itself becomes a major time cost if the thresholds and workflow are poorly tuned.
A comparison of scaling strategies for RPM data volume
Enterprise programs usually land in one of four models.
| Scaling approach | What it does well | What breaks first | Best fit |
|---|---|---|---|
| Manual review of all incoming readings | Fast to launch, low design overhead | Staffing cost, slow response consistency, alert fatigue | Pilot programs |
| Threshold-only alerting | Simple escalation logic, easy to explain | High false-positive volume, noisy work queues | Early production |
| Tiered triage with summaries | Reduces noise, matches staffing levels better | Requires data governance and workflow design | Multi-site health systems |
| Standards-based pipeline with FHIR normalization and analytics layer | Supports enterprise scale, EHR interoperability, reporting | Higher setup effort, stronger architecture discipline required | Mature RPM programs |
The pattern is clear: enterprise scale requires separation between raw data ingestion and clinician-facing action. If every incoming datapoint becomes a chart event, an alert, or a manual review task, the program eventually punishes its own adoption.
How enterprise teams usually control RPM data volume
The practical answer is not to suppress data blindly. It is to classify the data before it reaches the wrong queue.
1. Separate ingestion from intervention
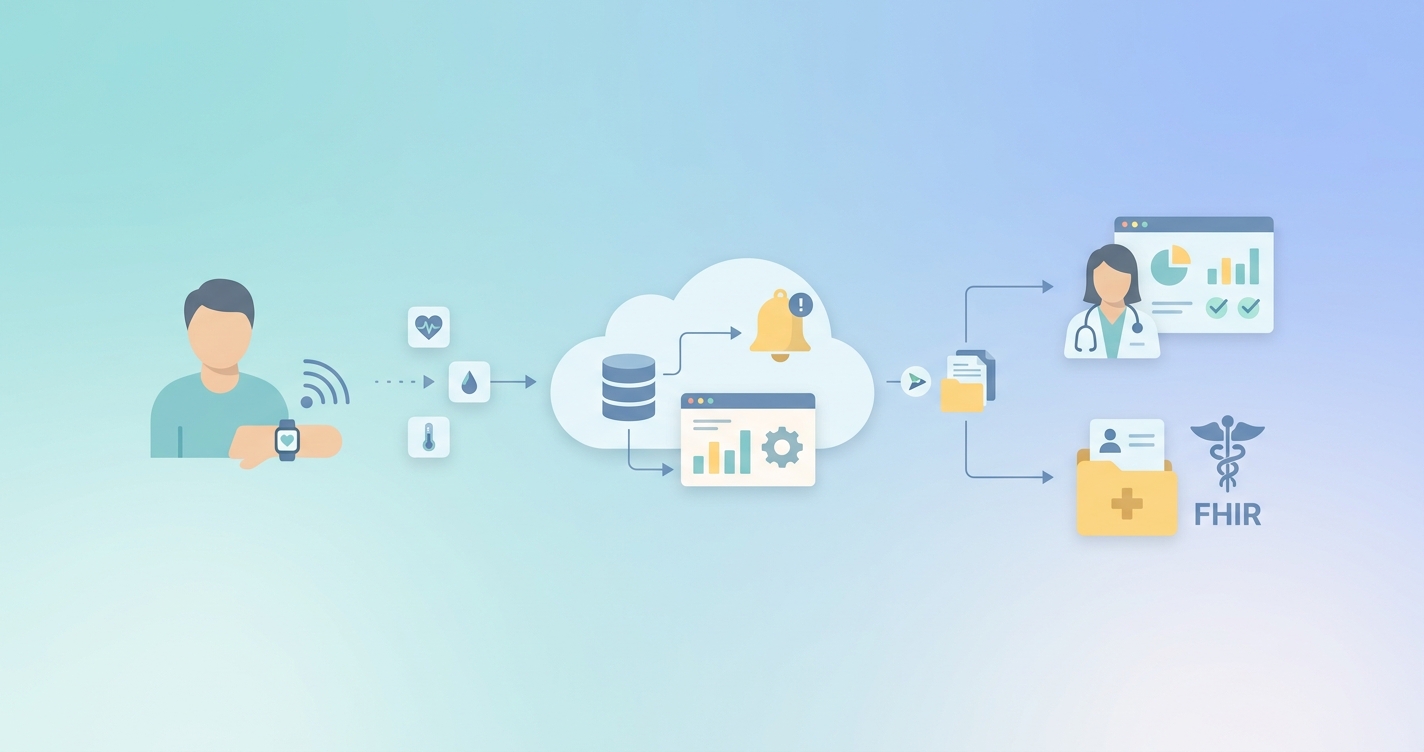
Raw device data should enter a durable intake layer first, not the clinician inbox. That intake layer can validate timestamps, units, patient identity, and device provenance before routing anything downstream. This is where FHIR helps. Standardized Observation, Device, and Patient resources create a cleaner handoff between RPM platform logic and EHR-facing workflows.
HL7's personal health device guidance for remote patient monitoring makes the same point in standards language: device-originated data needs context, provenance, and workflow-aware exchange, not just transport. For enterprise programs, that means treating FHIR as a normalization layer rather than a cosmetic API wrapper.
2. Promote summaries, not just single readings
Clinical teams do not usually need thousands of isolated values. They need trend context. A blood pressure spike matters differently if it is one noisy reading versus part of a three-day pattern. Enterprise RPM programs should calculate:
- Daily and weekly summaries
- Rolling averages and adherence rates
- Threshold persistence, not just threshold crossing
- Missing-data flags for nonadherence or connectivity issues
This reduces the number of transactions entering the EHR while improving clinical meaning.
3. Use tiered alerting instead of one-level thresholds
Van Steenkiste's 2025 study is useful here because it focuses on alert burden, not just technical throughput. The lesson is familiar to any operations team: if every abnormal reading is treated as equally urgent, the queue fills with low-value work. A tiered model works better:
- Informational events remain in the analytics layer
- Moderate-risk patterns create review tasks
- Persistent or severe events escalate into clinician alerts
That is a better fit for enterprise staffing models, especially when multiple service lines share one telehealth operations team.
Industry applications across enterprise RPM environments
Large integrated delivery networks
Integrated delivery networks care about consistency across hospitals, clinics, and home-based programs. Their challenge is not only volume but variation. Different departments often inherit different device vendors and alert rules. Enterprise-scale RPM architecture gives them a common intake and normalization model even when local workflows differ.
EHR integration teams
For integration teams, the core question is what belongs in the longitudinal record. Abdolkhani and colleagues pointed to lack of integration with EMR systems as one of the main barriers to confident clinical use of patient-generated health data. Enterprise teams need clear policies for when to write discrete observations, when to write summarized documentation, and when to retain data outside the chart but available on demand.
Telehealth operations groups
Operations leaders are usually the first to feel the consequences of bad data design. If alert queues rise faster than staffing capacity, response times slip and clinician trust erodes. The solution is not simply adding labor. It is reducing avoidable queue volume through rules, thresholds, routing, and service-line-specific escalation.
Population health and reporting teams
At enterprise scale, RPM data also feeds quality programs, utilization reviews, and contract reporting. That makes data quality non-negotiable. In their 2023 mixed-methods study in JMIR mHealth and uHealth, Robab Abdolkhani and coauthors proposed 19 recommendations across seven aspects of data quality management, arguing that the growth of wearable PGHD in RPM requires a systematic quality framework if the data is going to be trusted in care delivery.
Current research and evidence
The academic literature around RPM scale is converging on a few themes.
First, data quality remains a limiting factor. Abdolkhani, Gray, Borda, and DeSouza wrote in JAMIA Open (2019) that remote monitoring programs often lacked a clear data management or quality assurance approach. They identified digital health literacy, wearable accuracy, interpretation difficulty, and poor EMR integration as recurring obstacles.
Second, workflow design matters as much as clinical intent. In JMIR Medical Informatics (2025), van Steenkiste and colleagues studied a year of hypertension telemonitoring data and built a framework around alert reduction and process optimization. That work reflects a broader reality in enterprise RPM: handling the volume is less about database capacity than about reducing unnecessary review work.
Third, governance has to mature with scale. In JMIR mHealth and uHealth (2023), Abdolkhani and the same research group developed a guideline with 19 recommendations for quality management of patient-generated health data in RPM. The important point is that governance is not a side document. It is part of the architecture.
Outside the journal literature, ONC has continued pushing standards-based interoperability, and a recent ONC survey reported that 73% of surveyed digital health companies were already using standards-based APIs, primarily FHIR, for EHR integration. That does not solve RPM scale on its own, but it does show where enterprise architecture is headed.
The future of enterprise RPM data management
The next phase of RPM scale will probably look less like "more readings in more dashboards" and more like selective clinical compression. Health systems still need raw data retention, but they increasingly want the frontline workflow to focus on exceptions, trends, and documented interventions.
A few changes seem likely:
- More event-driven routing instead of blanket thresholding
- Greater use of FHIR-based normalization before EHR writeback
- More distinction between operational telemetry and chart-worthy clinical data
- Stronger patient-generated data quality controls at intake
- Wider use of analytics layers that summarize before escalating
That is good news for enterprise teams. The data volume problem is real, but it is not mysterious. Most of the failure modes are visible early: uncontrolled alert growth, weak provenance, inconsistent coding, and too much dependence on manual review.
Frequently asked questions
What is the biggest mistake organizations make when scaling RPM data?
Treating every incoming reading as a clinician-facing event. Enterprise programs need intake, normalization, summarization, and escalation layers. Without those layers, staffing pressure rises faster than patient volume.
Should every RPM reading be written into the EHR?
Usually no. Many organizations do better with selective writeback: discrete observations for clinically meaningful events, plus summaries and documentation for trend review. The right policy depends on service line, billing, and workflow needs.
Why does FHIR matter for RPM data volume?
FHIR does not reduce volume by itself, but it does standardize how data is represented and exchanged. That makes it easier to normalize device feeds, preserve provenance, and route the right information into EHR workflows.
How do enterprise teams reduce alert fatigue without missing risk?
They move from one-level thresholds to tiered triage. Persistent patterns, severe values, and multi-signal changes should escalate. Isolated low-confidence readings often belong in review or summary layers instead.
Enterprise RPM works better when the data pipeline is designed for clinical judgment instead of raw throughput. Teams evaluating how to scale standards-based intake, routing, and EHR integration can explore Circadify's telehealth workflow approach at circadify.com/solutions/telehealth?utm_source=usecarescan.com&utm_medium=microsite&utm_campaign=blog_cta. For related reading, see What Is HL7 FHIR? RPM Implementation Guide for Health IT and Interoperability Standards for Remote Monitoring Data: Overview.