7 Steps to Design a Telehealth RPM Workflow That Sticks
A 7-step blueprint for telehealth operations to design an RPM workflow clinicians actually adopt, from patient enrollment through clinical escalation.
Most remote monitoring programs do not fail because the devices stop working. They fail because the people meant to use them quietly stop. A nurse skips the morning queue when the alert list runs into the hundreds, a coordinator loses track of who enrolled last week, and a physician never trusts a reading that arrives outside the chart. Designing a telehealth RPM workflow that sticks is less a procurement exercise than an operational one, and the teams that treat it that way are the ones still running their programs two years later. This report lays out a seven-step blueprint for telehealth operations leaders who need clinicians to actually adopt the process rather than tolerate it.
Medicare RPM claims have grown by more than 3,000 percent since 2019, with reimbursements exceeding 500 million dollars in 2024, yet program-level retention remains the dominant operational risk for health systems scaling these services.
Why telehealth RPM workflow design decides adoption
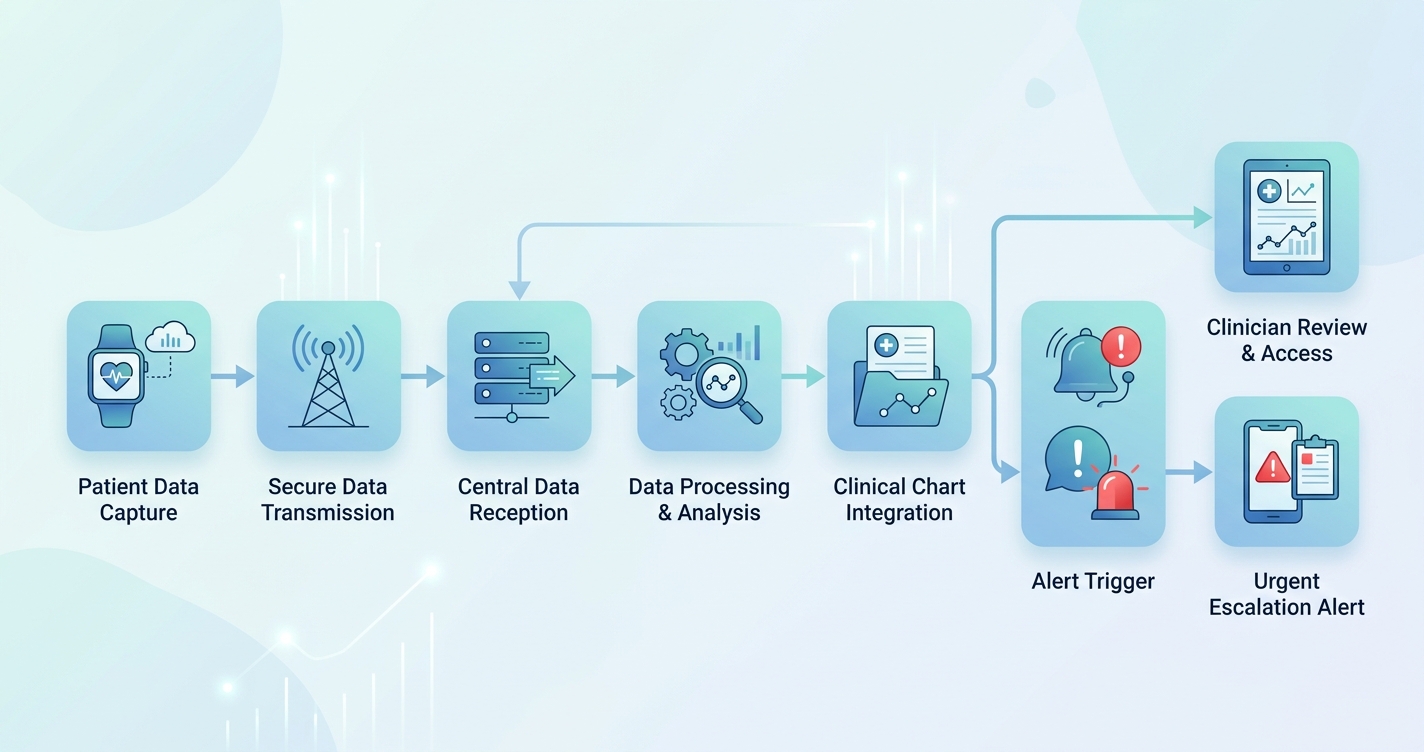
A telehealth RPM workflow is the end-to-end sequence that moves a patient from referral to enrolled participant, then routes their incoming vital signs to the right clinician at the right threshold, and finally closes the loop with documentation and billing. When that sequence is poorly mapped, the friction does not show up in a dashboard. It shows up as silent attrition: patients who stop measuring, staff who stop reviewing, and data that piles up unread.
A 2024 systematic review of clinical workflow adoption published in PMC (PMC10842520) found that the most consistent facilitators of RPM uptake were streamlined workflows, role clarity, and adequate clinician training, while the most consistent barriers were poor electronic health record integration and unclear escalation responsibility. In other words, adoption is an engineering problem with a human interface. Industry analyses put the patient appetite at roughly 30 million U.S. RPM users in 2024, rising from 23 million in 2020, so demand is not the constraint. Operational design is.
RPM clinical workflow design has to satisfy two audiences at once. The patient needs a process simple enough to repeat daily without a help desk call. The care team needs a process that fits inside existing EHR and telehealth tooling rather than asking them to live in a second screen. The seven steps below sequence those needs.
The seven steps at a glance
| Step | Workflow stage | Primary owner | Failure mode if skipped |
|---|---|---|---|
| 1 | Eligibility and referral logic | Telehealth operations | Wrong patients enrolled, low engagement |
| 2 | RPM patient enrollment workflow | Enrollment coordinator | Drop-off in first 14 days |
| 3 | Device provisioning and onboarding | Clinical support staff | Connectivity gaps, unusable data |
| 4 | Data ingestion and EHR integration | Health IT / EHR team | Readings stranded outside the chart |
| 5 | Threshold and triage rules | Clinical lead | Alert fatigue or missed events |
| 6 | Escalation and response pathways | Care team RPM workflow owner | Unclear accountability, slow response |
| 7 | Documentation and billing capture | Billing / compliance | Lost reimbursement, audit exposure |
Building each stage of the RPM patient enrollment workflow
The early steps carry the most adoption risk, because a patient who disengages in the first two weeks rarely returns.
- Step 1, Eligibility and referral logic. Define which conditions, payer mixes, and acuity levels qualify before a single device ships. Encode the criteria into the referral order so enrollment is not a judgment call made under time pressure. Hypertension and diabetes remain the highest-volume use cases, but the deciding factor is whether the patient can sustain a daily measurement habit.
- Step 2, RPM patient enrollment workflow. Treat enrollment as a designed conversation, not a form. Confirm consent, explain the measurement cadence, set expectations for who will call and when, and document a backup contact. Programs that automate outreach and scheduling at this stage reduce the coordinator burden that otherwise caps how many patients one team can carry.
- Step 3, Device provisioning and onboarding. The first reading is the highest-stakes moment in the entire telehealth remote monitoring process. If the patient cannot get a clean measurement on day one, confidence collapses. Cellular-enabled or app-light devices remove the home-network variable that generates the most early support tickets.
The middle of the workflow is where health IT ownership becomes decisive. Step 4, data ingestion and EHR integration, determines whether clinicians ever see the data inside the tools they already trust. Readings that arrive through an HL7 FHIR Observation feed land in the chart as structured, queryable values rather than as a PDF or a separate portal login. That distinction is the difference between a clinician glancing at a trend during a visit and a clinician ignoring the program entirely.
Industry applications across telehealth operations
Chronic disease management at scale
For hypertension and heart failure cohorts, the care team RPM workflow typically centers on a daily triage queue worked by nurses or medical assistants. The design goal is to keep that queue short enough to clear before noon. That requires upstream threshold tuning, not more staff. Programs report engagement gains when escalation rules are tuned to clinical significance rather than to raw out-of-range counts.
Post-acute and transitional care
Here the workflow is time-boxed. A 30 to 90 day monitoring window after discharge aims to catch decompensation early and reduce readmissions, which industry data associates with reductions of up to 25 percent in some chronic populations. The enrollment and onboarding steps must happen before discharge, because re-engaging a patient after they leave the building is far harder.
Distributed and rural telehealth networks
When patients are geographically dispersed, connectivity in Step 3 and ingestion reliability in Step 4 dominate the design. Offline-capable measurement with deferred upload protects data integrity when home internet is unreliable, so no reading is lost between the kitchen table and the chart.
Current research and evidence
The evidence base increasingly points to workflow, not hardware, as the determinant of program survival. The 2024 PMC systematic review of clinician perspectives identified unclear escalation responsibility as a recurring failure point, reinforcing why Steps 5 and 6 deserve explicit role mapping rather than informal habit. Separately, market and utilization analyses compiled across 2024 reporting show RPM patient counts approaching 30 million in the United States and Medicare reimbursement crossing 500 million dollars, signaling that the financial model now rewards programs that can retain patients long enough to bill consistent monitoring periods.
What the data does not yet standardize is alert design. Alert fatigue remains the most cited reason clinicians disengage from a triage queue, and the corrective is threshold logic that prioritizes by clinical risk and trend rather than single out-of-range values. Teams that audit their alert-to-action ratio monthly tend to keep clinician trust intact, while teams that never measure it tend to watch review rates decay.
The future of telehealth RPM workflow design
Three shifts are reshaping how these workflows will be built over the next few years. First, integration is moving from custom interfaces to standards-based FHIR pipelines, which lowers the engineering cost of routing vital signs into any compliant EHR. Second, triage is becoming risk-stratified by default, with decision support filtering the queue before a human ever sees it, so the daily list reflects clinical priority rather than data volume. Third, enrollment is becoming continuous rather than campaign-based, with eligibility logic embedded in the referral order so patients flow into the program as a routine part of care.
The common thread is that the workflow itself, not any single device or vendor, becomes the durable asset. A program designed around clean enrollment, structured ingestion, tuned thresholds, and accountable escalation can swap components without disrupting the people who run it. That is what makes a telehealth RPM workflow stick.
Frequently asked questions
What is a telehealth RPM workflow? It is the end-to-end operational sequence that moves a patient from referral and enrollment through device onboarding, data ingestion into the EHR, threshold-based triage, clinical escalation, and finally documentation and billing. A well-designed workflow keeps each stage owned by a defined role so nothing falls between the gaps.
Why do RPM programs lose patients in the first two weeks? Early attrition usually traces back to the enrollment and onboarding steps. If consent and expectations are rushed, or if the first home reading fails because of connectivity or device confusion, patients lose confidence and stop measuring. Designing Steps 2 and 3 carefully protects long-term engagement.
How does EHR integration affect clinician adoption? Clinicians adopt RPM when the data appears inside the chart they already use. Routing readings through an HL7 FHIR Observation feed delivers structured, queryable values rather than a separate portal or PDF, which removes the extra-screen friction that causes care teams to ignore a program.
How do you prevent alert fatigue in the care team RPM workflow? Tune escalation thresholds to clinical significance and trend rather than to raw out-of-range counts, and audit the alert-to-action ratio regularly. A triage queue short enough to clear in a morning is the practical signal that the rules are working.
Circadify is addressing this space directly, building HL7 FHIR compatible RPM data pipelines that plug into existing EHR and telehealth tooling so your seven-step workflow runs inside the systems clinicians already trust. Telehealth operations teams can review the integration documentation and EHR guides, or book a workflow design consultation, at circadify.com/solutions/telehealth.