How to Validate FHIR Vital Signs Data Before the EHR
A technical guide for EHR integration teams on validating and cleaning FHIR vital signs data so erroneous RPM readings never reach the patient chart.
The chart is the point of no return. Once a remote patient monitoring (RPM) reading lands in the EHR as a clinical observation, it carries the same authority as a measurement taken at the bedside. It triggers alerts, informs medication titration, and becomes part of the legal record. That is precisely why the validation layer that sits in front of the EHR matters more than any single device specification. For integration teams, the discipline of inspecting FHIR vital signs data before it persists is the difference between a feed clinicians trust and one they quietly ignore.
The problem is not theoretical. RPM feeds carry a measurable share of malformed, out-of-range, and improperly coded observations, and the FHIR transport layer does not clean them for you. A resource can be perfectly well-formed JSON, pass schema parsing, and still describe a diastolic pressure of 400 mmHg or a temperature missing its UCUM unit. Catching that before write time is an engineering responsibility, not a clinical one.
A study of hospitalized patients using a wireless vital signs monitor reported that 10.8% of SpO2, 10.2% of pulse rate, 13.4% of temperature, and 11.1% of respiratory rate data points had to be excluded due to missing or invalid measurements from unstable signal quality (Boillat et al., wireless vital signs validation study, PMC).
Why FHIR vital signs data needs a validation gate
Validating FHIR vital signs data means more than confirming the payload parses. The HL7 FHIR US Core Vital Signs Profile, built on the base FHIR R4 vital signs profile, defines a minimum set of constraints every Observation must satisfy: a status, a category of vital-signs, a subject reference to the patient, a clinically relevant effectiveDateTime, a LOINC code identifying what was measured, and a UCUM unit for any numeric result. A resource that omits any of these is non-conformant, even if the receiving server accepts it.
But conformance is only the first of several gates. Profile validation tells you the structure is correct. It says nothing about whether the value is physiologically plausible, whether the code maps to the right flowsheet row, or whether this reading is a duplicate of one ingested ten seconds earlier. Robust FHIR observation validation layers these checks in sequence so that bad readings fail closed rather than flowing through.
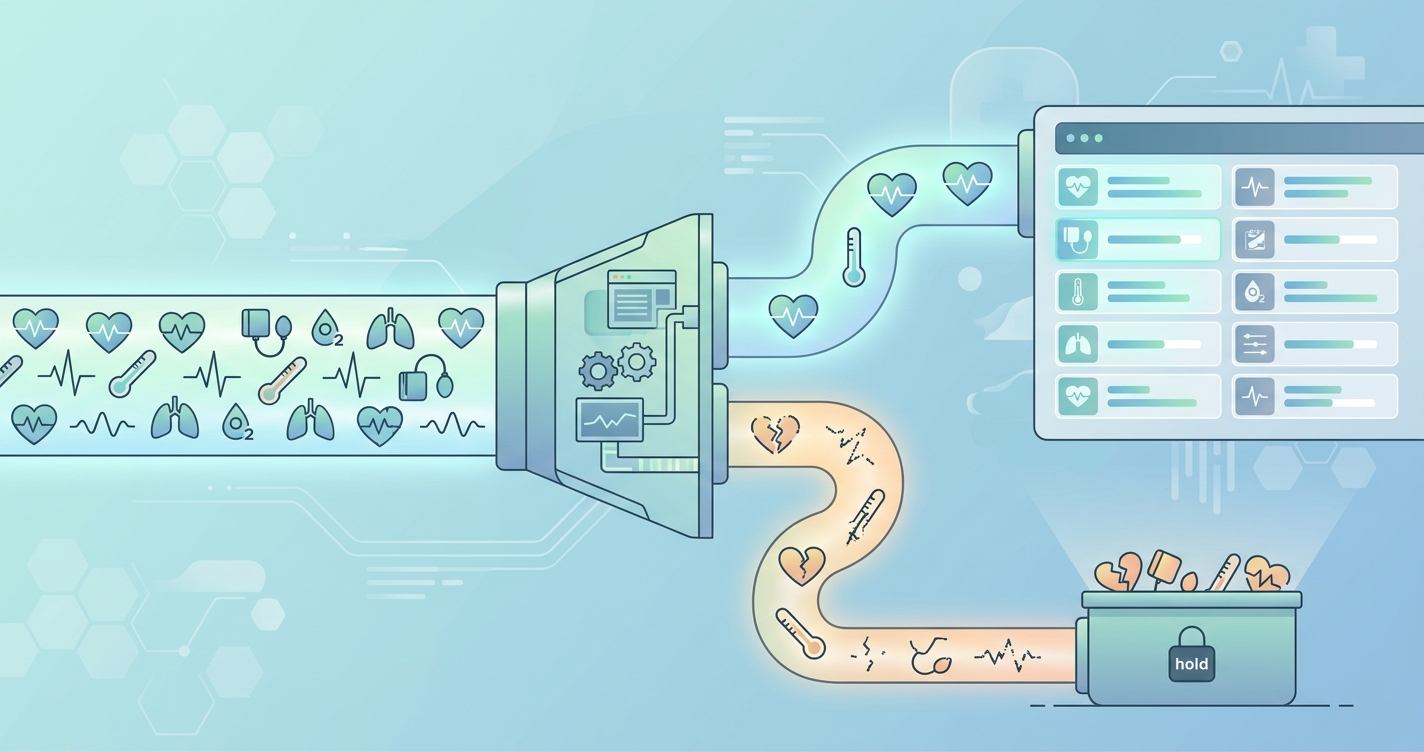
A practical validation gate inspects each incoming Observation across four independent dimensions:
- Structural conformance - does the resource validate against the US Core Vital Signs Profile (LOINC present, UCUM unit present, required elements populated)?
- Semantic correctness - does the LOINC code match the unit and the expected component structure (for example, blood pressure as a panel with systolic and diastolic components)?
- Physiological plausibility - does the numeric value fall within a defensible range for that vital sign and patient cohort?
- Provenance and integrity - is the device source identified, the timestamp sane, and the reading not a duplicate or a backfilled artifact?
A comparison of validation approaches
Integration teams generally choose between three architectures for cleaning an RPM feed. Each trades implementation effort against the strength of the guarantee it offers the EHR.
| Validation approach | What it catches | What it misses | Latency cost | Best fit |
|---|---|---|---|---|
| EHR-native intake rules only | Gross schema errors, missing required fields | Plausibility errors, bad code-to-unit mapping, duplicates | Low | Small single-vendor pilots |
| FHIR profile validator (US Core) | Structural non-conformance, missing LOINC/UCUM | Out-of-range values, semantic mismatches, provenance gaps | Low to moderate | Teams standardizing on US Core |
| Dedicated pre-EHR validation pipeline | Conformance, plausibility, semantic, duplicate, and provenance errors | Device-level sensor inaccuracy (must be flagged upstream) | Moderate | Multi-vendor RPM at scale |
The pattern that holds up at enterprise scale is the dedicated pipeline. It treats validation as a discrete stage between ingestion and persistence, where each Observation is scored, tagged, and either passed, quarantined, or rejected with a structured reason code that downstream teams can audit.
Building the validation pipeline
A clean RPM data feed is engineered, not assumed. The pipeline below reflects how teams sequence checks to fail fast and preserve auditability.
Stage one: structural and profile validation
Run every Observation through a FHIR validator configured against the US Core Vital Signs Profile (current implementation guides reference LOINC 2.70 and UCUM Revision 2.1). Reject resources missing a LOINC code, a UCUM unit on numeric values, the vital-signs category, or the patient reference. This stage is deterministic and should be fully automated.
Stage two: semantic and mapping validation
Structural validity does not guarantee correct meaning. This is where vital signs data mapping earns its keep. Confirm that the LOINC code and the unit agree: a heart rate coded as 8867-4 should carry /min, not mmHg. Blood pressure should arrive as a panel (LOINC 85354-9) with systolic and diastolic components rather than two unlinked observations. A mismatch here routes a reading to the wrong flowsheet row, which is more dangerous than an outright rejection because it looks correct on the chart.
Stage three: physiological plausibility
Apply range gates per vital sign. Home blood pressure devices alone are inaccurate in 5% to 15% of patients depending on the threshold applied, so plausibility filtering is non-negotiable for RPM data integrity. Define hard limits (impossible values, rejected outright) and soft limits (improbable values, quarantined for review). The goal is not to silently discard data but to prevent an artifact from triggering a false clinical alert.
Stage four: provenance, deduplication, and timestamps
Confirm each Observation references a known device, carries a plausible effectiveDateTime, and is not a duplicate of an existing reading. Backfilled data after a connectivity outage is legitimate but must be timestamped to when the measurement occurred, not when it arrived, so trend lines stay accurate.
Industry Applications
Multi-vendor RPM programs
Health systems running blood pressure cuffs, pulse oximeters, and weight scales from several manufacturers face inconsistent coding and unit conventions across vendors. A pre-EHR validation layer normalizes all of it to US Core before write time, which is the only sustainable way to keep a clean RPM data feed across a heterogeneous device fleet.
Telehealth operations and alert management
The same evidence that justifies plausibility filtering explains alert fatigue. When erroneous readings reach clinical decision support, they generate false alarms that erode trust. Validating FHIR vital signs data upstream keeps the alert queue populated with signal, not noise.
Compliance and audit readiness
Every rejected or quarantined Observation should carry a structured reason code and a retained copy. This audit trail supports both data governance reviews and the documentation requirements tied to reimbursed RPM services.
Current research and evidence
The case for upstream validation rests on documented error rates rather than vendor assurances. The wireless monitor study cited above found that roughly one in nine readings across SpO2, pulse, temperature, and respiratory rate were unusable due to unstable signal quality. Separately, research on documentation methods found an 18.75% error rate for manual paper-to-EMR transcription versus a 0% error rate for an automated wireless pathway, evidence that automation removes a large class of human transcription errors but shifts the burden to validating machine-generated data instead (Eliminating Errors in Vital Signs Documentation, CEConnection for Nursing).
Validation studies of contactless and telehealth-based vital sign capture have reported mean absolute percentage differences of 1.69% for heart rate, 0.59% for oxygen saturation, and 4.72% for respiratory rate against reference measurements. Those figures are encouraging for the median reading but say nothing about the tail of artifacts, which is exactly what a validation gate exists to catch. The consistent finding across this literature is that device accuracy and feed integrity are separate problems, and only the second can be solved at the integration layer.
The Future of FHIR vital signs data validation
Three shifts are reshaping how teams approach validation. First, FHIR Subscriptions and bulk data export are pushing validation toward streaming rather than batch processing, which means plausibility and conformance checks must run inline at ingestion speed. Second, profile tooling is maturing: machine-readable US Core profiles let teams version their validation rules alongside the implementation guide rather than hard-coding thresholds. Third, provenance is becoming a first-class requirement, with device attribution and timestamp integrity treated as validation criteria rather than metadata afterthoughts. The direction of travel is clear. Validation is moving from an optional safeguard to a standard stage in the RPM data path, owned by integration teams and measured like any other reliability metric.
Frequently asked questions
What is the difference between FHIR validation and FHIR vital signs validation? FHIR validation confirms a resource is structurally well-formed and conforms to a profile such as US Core Vital Signs. Vital signs validation adds clinical and operational checks on top: physiological plausibility, correct LOINC-to-unit mapping, deduplication, and provenance. A reading can pass structural validation and still be clinically implausible.
Should invalid readings be deleted or kept? Quarantine rather than delete. Rejected and quarantined observations should be retained with a structured reason code so the data can be reviewed, audited, and reprocessed if a rule was too strict. Silent deletion destroys the audit trail that data governance and reimbursement reviews depend on.
Where should the validation layer live? Between ingestion and EHR persistence, as a discrete pipeline stage. Relying solely on EHR-native intake rules catches gross errors but misses plausibility, mapping, and duplicate problems. A dedicated pre-EHR layer gives you a single place to enforce US Core conformance across every device vendor.
How do I keep validation from delaying urgent readings? Run deterministic structural and plausibility checks inline at low latency, and reserve human review only for quarantined edge cases. Hard-limit rejections and pass decisions happen in milliseconds, so genuinely urgent readings reach the chart without added delay.
Circadify is building toward this exact problem, treating validation and normalization as a first-class stage in the RPM data path rather than an afterthought bolted onto the EHR. Health IT teams evaluating how to harden their incoming feed can review the integration documentation and EHR guides at circadify.com/solutions/telehealth to see how a HL7 FHIR-compatible pipeline keeps bad readings off the chart.